Uterine abnormality - problems with the womb
Some women have a womb (uterus) that is different in shape or size from the norm. This is called abnormality of the womb or congenital uterine abnormality. It means that your womb (uterus) formed in an unusual way before you were born.
Many women have a differently shaped womb but are unaware as there often aren’t any symptoms. You may only find out during an ultrasound scan or if you’ve experienced miscarriage, bleeding or difficulties conceiving. Some women have told us that knowing about a womb abnormality has helped them to plan and prepare for pregnancy.
Although these abnormalities are quite common, the effect they have on pregnancy isn’t always clear. Having a womb abnormality won’t always affect your ability to become pregnant, but it may be more difficult for you to carry your baby to full-term. Depending on the shape of the womb, there may be an increased risk of miscarriage or preterm birth (giving birth before 37 weeks). Womb abnormality can also be linked to a weaker cervix (sometimes called cervical incompetence), which can lead to preterm birth. You may need extra monitoring during pregnancy to keep you and your baby safe.
On this page, we explain the different types of womb abnormalities and the effects they may have on pregnancy. Reading about these increased risks may be scary but try to remember that many women do manage to get pregnant and have a healthy baby. Your healthcare team will be able to support you throughout your pregnancy to help reduce any risks.
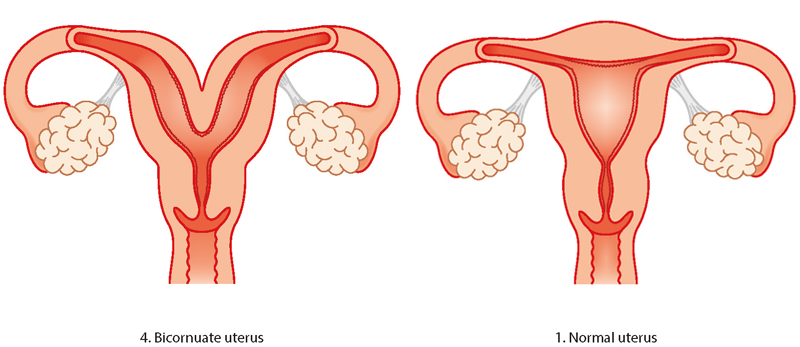
Bicornuate womb
A bicornuate womb has a deep indentation at the top. Women with a bicornuate womb have no extra difficulties with conception or in early pregnancy, but there is a slightly higher risk of miscarriage and preterm birth. It can also affect the baby’s position later in the pregnancy so a c-section (caesarean) might be recommended.
Unicornuate womb
Having a unicornate womb is rare. It means your womb is half the size of a normal womb because one side didn’t develop. There is an increased risk of ectopic pregnancy (an abnormal pregnancy that implants and develops outside the womb), late miscarriage or preterm birth. The baby may lie in an awkward position in later pregnancy so a c-section (caesarean) might be recommended. Women who have unicornate wombs can conceive, although unicornuate wombs are more common in women who are infertile.

Didelphic (double) womb
The didelphic womb is split in two, with each side having its own cavity. This usually affects the womb and cervix, but it can also affect the vulva, bladder, urethra and vagina. Women with a didelphic womb have no extra difficulties with conception and it is only linked to a small increase in the risk of preterm birth.

Septate/subseptate womb
A septate womb has a wall of muscle coming down the centre splitting the space in two. Sometimes the wall only comes part-way down the womb (subseptate) and other times it comes the whole way down (septate). Women with subseptate or septate wombs are more likely to have difficulties with conception. There is also an increased risk of early miscarriage and preterm birth. In later pregnancy, the baby may not be lying in a head-down (cephalic) position so you may be advised to have a c-section.

“When I was first diagnosed with a septate uterus, I was petrified. I read a lot of scary information online about the risks associated with a septate uterus. My consultant reassured me that a lot of women have congenital uterine abnormalities and are not aware. I read online that a lot of women with a septate uterus have surgery to resect the septum before pregnancy. My consultant did not recommend this. Despite having a complete septate uterus, I was able to carry my baby to term. He was breech, so I did have an elective c-section. I wish I would have trusted my consultant more and not believed everything I read online.”
Emma
Arcuate womb
The arcuate womb looks very like a normal womb but it has a dip at the top. Having an arcuate womb doesn’t increase your risk of preterm birth or early miscarriage but it may increase your risk of late miscarriage. In later pregnancy, your baby may not be lying head down so you may need to have a c-section.

Review dates
